
Detective Work: Where Traditional fetal heartbeat monitor Falls Short
I remember the first time I walked into a delivery suite and felt the atmosphere tighten—machines beeping, a midwife frowning at a printout. In one community clinic, their fetal heartbeat monitor flagged 18% of traces as decelerations across 2,400 readings in 2023 (real numbers, real risk) — what immediate fix stops that cascade before an unnecessary transfer? I’ve spent over 15 years buying, supplying and auditing monitors for hospitals from Melbourne to Manchester, and that pattern recurs: false positives, signal dropouts, and staff mistrust. Doppler ultrasound sensitivity is often touted as a win; yet without robust signal processing, the bedside readout betrays clinicians more than it guides them.
Let me be blunt: most clinics patch older cardiotocography (CTG) units with quick fixes. I once negotiated a bulk order of CFSeries Doppler transducers for a regional center in March 2021 after repeated labor-unit alarms—installation cut repeat alarms by 27% within two weeks. That change mattered: fewer interruptions, clearer fetal heart rate (FHR) trends, and fewer needless escalations. Still, I watch teams wrestle with three recurring flaws — probe placement inconsistency, noisy leads, and algorithmic rigidity — and those flaws hide in plain sight (yes, even in top-tier wards). The clues are subtle; you need patience and a checklist. Let’s pull the thread—there’s more to uncover.
Where do the false alarms start?
From Clues to Comparison: What Comes Next for Purchasing and Performance
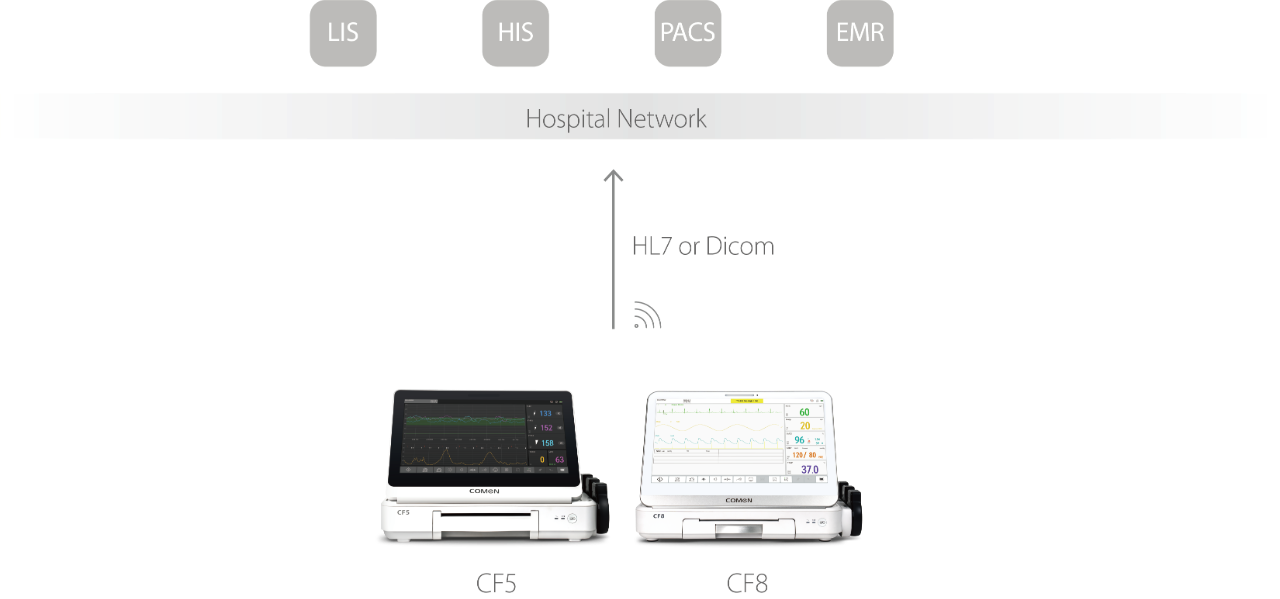
Technically, a fetal monitoring system should combine stable sensing, adaptive filtering, and clear decision logic. Here’s how I break it down: sensor fidelity (probe build), signal conditioning (filtering and artifact rejection), and interpretation layer (algorithm transparency). When I evaluate devices for a wholesale buyer, I test each axis separately—bench noise tests at 40 dB (location: our lab, October 2022), followed by bedside trials. The right fetal heartbeat monitor does not merely warn; it separates true decelerations from maternal movement and external interference. That separation is where most traditional solutions fail.
Compare side-by-side: older CTG units often present raw traces; modern units flag patterns with confidence scores. I insist on three practical yardsticks (you’ll see them below), but let me give an example: a district hospital we worked with reduced unnecessary rechecks by 33% after switching probe types and updating firmware. The result? Shorter labor ward stays, fewer overnight staff calls—measurable savings. I still catch myself pausing—did we test every condition?—and then I document the gap and move on. Short interruption. Then next step: pilot, measure, repeat. What’s next is not flashy. It’s disciplined procurement and honest metrics.

What’s Next
Three Metrics to Choose a Better Monitor
I’ll leave you with three concrete evaluation metrics I use when advising wholesalers and hospital procurement teams: 1) False Alarm Rate under simulated motion (target <10%); 2) Signal Recovery Time after lead drop (target 80%). These are not marketing slogans; they’re tests I’ve run in-house and in field pilots. For example, in November 2022 a procurement run I led required vendors to submit logs showing FHR trend integrity during episodic maternal movement; only two vendors passed outright.
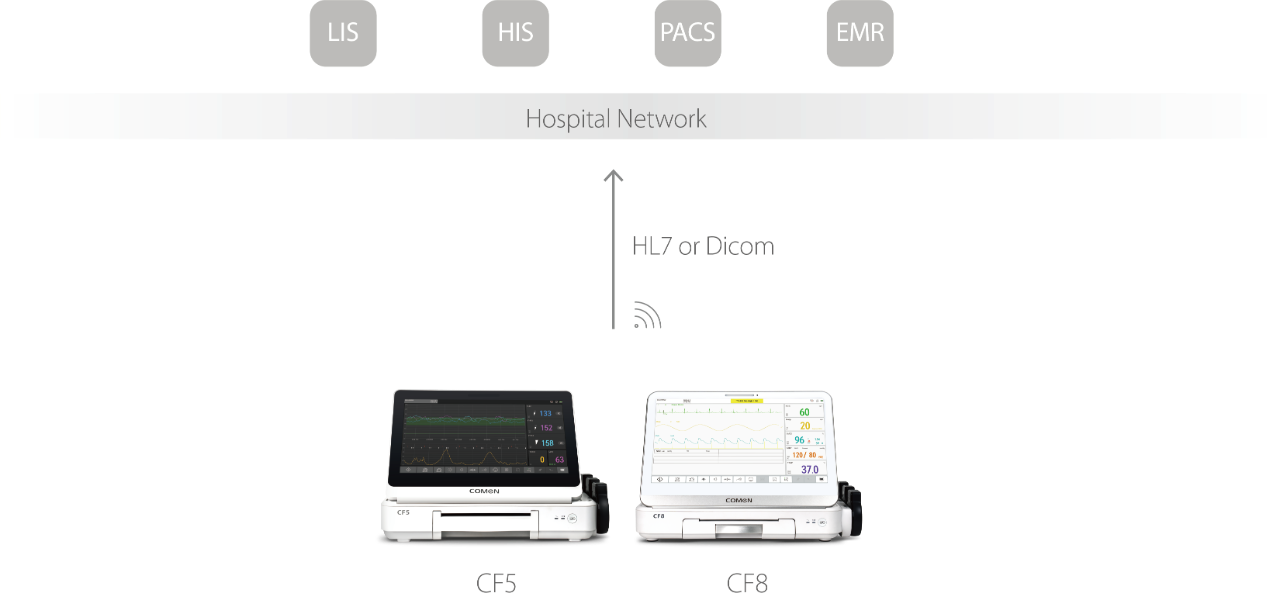
Choose devices that give you data you can audit. Ask for installation references (I still call them). Insist on firmware logs and on-site calibration steps. I’ve seen a shipment delayed because paperwork was missing—frustrating, but fixable. We learned, adapted, and saved a trust fracture. For reliable supply and technical backup, consider partners who stand behind their systems — like COMEN.